Highlights
- Patients with no binocular vision dysfunction generally adapt to prisms, as they have a normally functioning vergence mechanism.
- Patients who are symptomatic are less likely to adapt to prism and will benefit from a prism correction.
- 6 out of 10 Neurolens wearers did not show any significant sign of prism adaptation.
- The mean change in the Neurolens prism prescription was less than 1/3rd of a prism diopter over time and the stability of the Neurolens prism prescription improved over time.
Vergence Mechanism and Prism Corrections
Optical prisms are one of the most commonly employed treatment modalities to correct binocular (vergence) dysfunctions involving eye misalignments, including heterophorias, fixation disparities and tropias. There is an inter-clinician variability in prism prescribing guidelines which is driven by factors such as clinicians’ opinion or knowledge on prism corrections and binocular vision. There is anecdotal clinical evidence on the efficacy of prism treatment on patients with various binocular dysfunctions. Some clinicians also argue that prism corrections are not good given an individual’s ability to adapt to prism corrections. This lack of consensus is coupled with a lack of evidence-based clinical standards on how to effectively use prisms to correct binocular dysfunctions1. There are three main reasons why a prism correction tends to be unstable: (i) individual differences in a person’s innate ability to adapt to a prism; (ii) presence of a latent eye misalignment that may not have been detected during the initial eye examination; and (iii) our inability to measure an accurate and repeatable clinical parameter that assesses the vergence mechanism and consistently represents the symptomatology experienced by the patient.
The vergence system is unique, in terms of its cross-coupled relationship with the accommodative mechanism and its ability to adapt naturally. Broadly speaking, an alignment response to a stimulus in the real world comprises of outputs from two components of the vergence mechanism: a fast (reflex) and a slow (adaptive) responding controller. Although the neural correlations of the two components are not well established, several experimental studies confirmed their response patterns along with their temporal characteristics2. When a person shifts their fixation from distance to near, the initial response to that new object of interest is initiated by the reflex system. If the near fixation is prolonged, the slow adaptive system takes over the response to maintain alignment without any perceivable discomfort. Previous studies have reported that the strength/magnitude of the response of this slow adaptive component often correlates with the presence of symptomology in patients with binocular vision dysfunction (BVD)3.
The ability to adapt to prism also correlates with this overall ability to adapt3. In other words, people with a better functioning adaptive controller tend to adapt more to prism corrections. Patients with no binocular vision dysfunction generally adapt to prisms, as these patients tend not to be symptomatic and have a normally functioning vergence mechanism3. However, patients who are symptomatic are far less likely to adapt to prism and far more likely to benefit from prism correction3, 4. That said, it is critical to remember that some patients may have latent deviations that require more than one prism correction before they are completely compensated and stable. In fact, a previous study reported that about 80% of individuals in a sample of 46 symptomatic subjects adapted to a standard prism and needed a change in their prescription over the next few years5.
Furthermore, clinicians tend to use subjective and imprecise techniques to measure patients’ binocular vision, including phoria, fixation disparity or fusional vergence. Some practitioners measure any one of these parameters to decide the corrective option while others tend to employ a combination of measurements before deciding the appropriate treatment for their patient’s condition. Multiple studies have concluded that none of these clinical measurements correlated well with the subjective symptomology experienced by the patients6. This combination of inconsistent clinical practices, inability to accurately measure and represent patients’ symptoms and variability in an individual’s ability to adapt to a prism would leave the clinician with a lot of unanswered questions, making them hesitant to prescribe a prismatic correction to their patient. It also raises two critical questions:
- What is the best way to identify and treat patients with BVD?
- If there is a better way, do we have evidence to understand if—and to what extent—prism adaptation contributes to this issue?
The Neurolens process: a better way to do BV testing

Figure 1: The Neurolens process
The Neurolens process consists of three major components: a lifestyle index, a Neurolens measurement and a Neurolens correction (figure 1). Potential patients who can benefit from a Neurolens correction will first be identified using a simple questionnaire (Neurolens lifestyle index) which quantifies common symptoms associated with a binocular vision dysfunction, such as headaches. Symptomatic patients would then undergo an eye alignment measurement using the Neurolens Measurement Device (NMD).
The NMD is an objective, accurate, precise, simple and efficient way to measure eye alignment and calculate a patient’s AC/A7. The NMD does not rely on subjective responses, thereby eliminating both clinician and patient biases or variabilities. The objective measurement of the NMD is achieved by employing an eye tracking system that robustly tracks patients’ eyes in a continuous fashion while the eyes are being dissociated and associated. The NMD is simple in the sense that it employs an iterative procedure, which takes the misalignment measurements into account and provides a final Neurolens prism correction (Neurolens value). Unlike prescribing guidelines such as Sheard’s Criterion, Percival’s Rule or the 1:1 rule, the Neurolens value utilizes a proprietary algorithm that was developed based on patient outcomes across hundreds of thousands of measurements. The Neurolens value obtained by the NMD represents the distance prismatic correction that can be readily used by clinicians to treat their patients.
Neurolens correction involves a proprietary contoured lens design which seamlessly varies the prismatic correction provided to the eyes at different distances. This design allows clinicians to treat their patients with a distance prism correction and additional correction at near. Given that Neurolens doesn’t provide the same prismatic correction across the lens—thereby eliminating the need to over-prescribe at distance to receive an appropriate correction at near—it is reasonable to expect that a patient’s likelihood to adapt to this prism would also be limited. The Neurolens process provides a simple and repeatable way to assess binocular vision and treat patients with confidence.
Commercial Data
To test the above hypothesis that patients are less likely to adapt to Neurolens contoured prism correction, commercial data was collected from Neurolens wearers who had at least one follow-up measurement, with at least one year having elapsed between the initial visit and the follow-up visit. A total of 1,183 Neurolens wearers that met these criteria were evaluated. 182 of these individuals had two follow-ups, and 30 had three follow-ups since receiving their initial Neurolens prescription.
Refractive and prism prescription after one follow-up
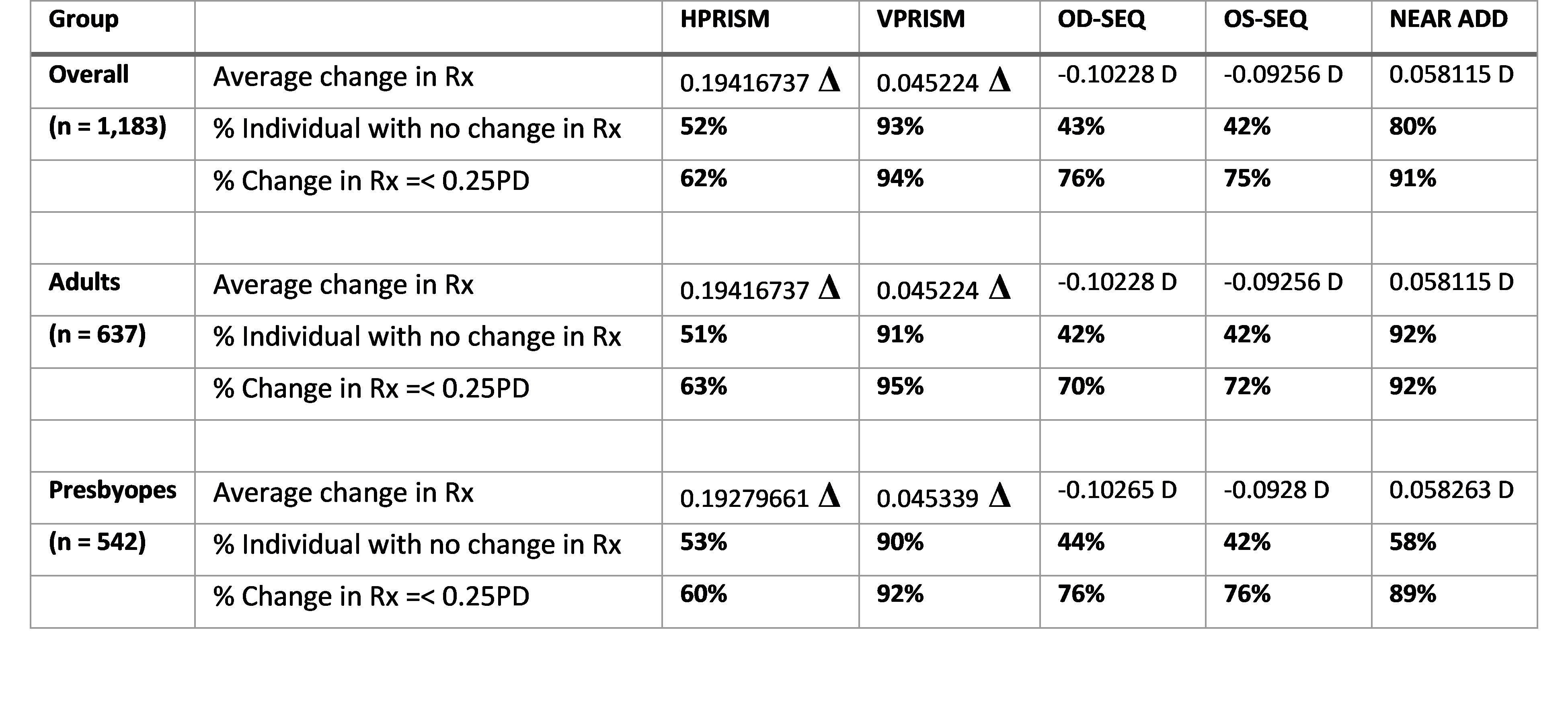 52% individuals showed no change in their horizontal prism prescription; surprisingly, this was more stable than the percentage of individuals who showed no change in refractive error. There was not a significant difference in prism adaptation as a function of age; but overall, more presbyopes had no change in the prescription at the follow up visit. Overall, vertical prism prescription remained stable in over 90% of individuals.
52% individuals showed no change in their horizontal prism prescription; surprisingly, this was more stable than the percentage of individuals who showed no change in refractive error. There was not a significant difference in prism adaptation as a function of age; but overall, more presbyopes had no change in the prescription at the follow up visit. Overall, vertical prism prescription remained stable in over 90% of individuals.
Refractive and prism prescription after two or three follow-ups
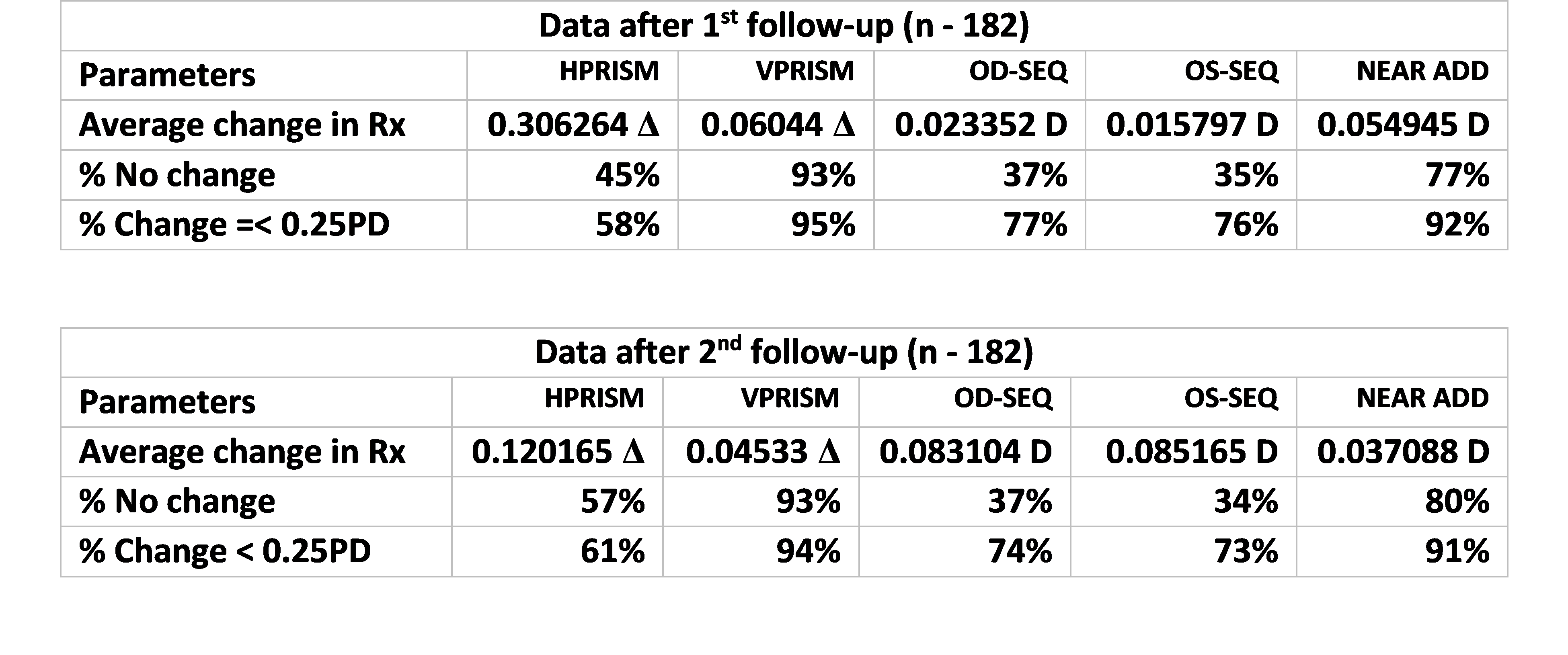 45% individuals showed no change in their horizontal prism prescription at the first follow-up and that number improved 57% at the second follow-up, suggesting that the stability of the prescription improved over time. As shown before, prism prescription stability was better than the stability of the refractive error prescription. Overall, vertical prism prescription remained more stable in over 90% individuals.
45% individuals showed no change in their horizontal prism prescription at the first follow-up and that number improved 57% at the second follow-up, suggesting that the stability of the prescription improved over time. As shown before, prism prescription stability was better than the stability of the refractive error prescription. Overall, vertical prism prescription remained more stable in over 90% individuals.
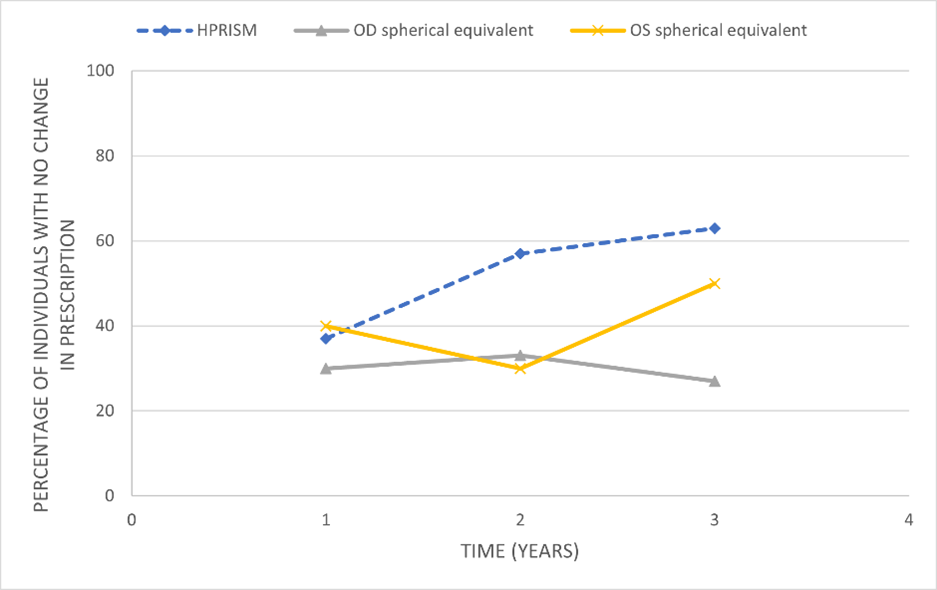
Figure 2: Percentage of individuals no change in horizontal prism (dotted blue line), along with OD and OS spherical equivalent (OD - grey and OS- yellow) were plotted as a function of time.
Evaluating those with three follow-ups since their initial Neurolens prescription, 37% of these individuals showed no change in their horizontal prism prescription at the first follow-up; that number improved 57% at the second follow-up and 63% at the third follow-up, further supporting increased stability from visit to visit. The mean change in the prism prescription was less than 1/10th of a prism diopter over time. As shown before, prism prescription stability was better than the stability of the refractive error prescription, which was found to be as low as 27-50% across different follow up visits.
Discussion and Conclusion
Unlike previous studies on prism adaptation5, commercial Neurolens data collected from individual eyecare practices across the country indicate that only 48% of patients who received a Neurolens correction for the first time had a change in their Neurolens prescription at their first follow-up (after 1 or 2 years). It is important to remember that this change in prescription could be due to emergence of the latent deviation in the patient not detected during the initial testing. The stability of the Neurolens prescription improves over time, suggesting the eye misalignment—both manifest and latent—is accurately compensated over time. This could also indicate a change in the individual’s vergence posture due to either an improving fusional vergence mechanism or prism adaptation. 80-85% of the patients who provided us a 60-day follow-up symptomology survey reported relief in their symptoms after wearing Neurolens and were willing to recommend Neurolens to their friends and family. Therefore, we believe that most of these patients who reported symptom relief post Neurolens wear had an improved fusional vergence mechanism.
So, do patients adapt to a Neurolens correction? Approximately 6 out of 10 patients did not show any sign of adaptation to a Neurolens correction as of their second follow-up. This is significantly lower than the adaptation frequency reported in the previous study (80%)4, suggesting that the Neurolens process is more stable and effective than a standard prismatic correction calculated based on the traditional prescribing guidelines. As has been shown time after time, prism is a very effective optical tool used to relieve symptomology associated with binocular vision dysfunction. Given the lack of consensus on measurement and treatment guidelines, it is not surprising that most clinicians are hesitant to provide prismatic corrections to their patients who are likely to benefit from the treatment. The Neurolens Measurement Device (NMD), coupled with a customizable contoured prism design, provides a comprehensive and straightforward way to accurately diagnose and treat binocular vision dysfunction.
References
1. Gray, L. S. (2008). The prescribing of prisms in clinical practice. Graefe's Archive for Clinical and Experimental Ophthalmology, 246(5), 627-629.
2. Schor, C. M. (1992). A dynamic model of cross-coupling between accommodation and convergence: simulations of step and frequency responses. Optometry and vision science: official publication of the American Academy of Optometry, 69(4), 258-269.
3. Schor CM. The relationship between fusional vergence eye movements and fixation disparity. Vision Res 1979; 19:1359–1367.
4. North R, Henson DB. Adaptation to prism induced heterophoria in subjects with abnormal binocular vision or asthenopia. Am J Optom Physiol Opt 1981; 58:746–752.
5. Lie, I., & Opheim, A. (1985). Long-term acceptance of prisms by heterophorics. Journal of the American Optometric Association, 56(4), 272–278.
6. Sheedy JE, Saladin JJ (1983) Validity of diagnostic criteria and case analysis in binocular vision disorders. In: Schor CM, Ciuffreda KJ (eds) Vergence eye movements: basic and clinical aspects. Butterworths, Boston.
7. Labhishetty V., (2020) Factors contributing to the inaccuracy and lack of repeatability with the traditional subjective heterophoria measurements.